





Shoulder Separation
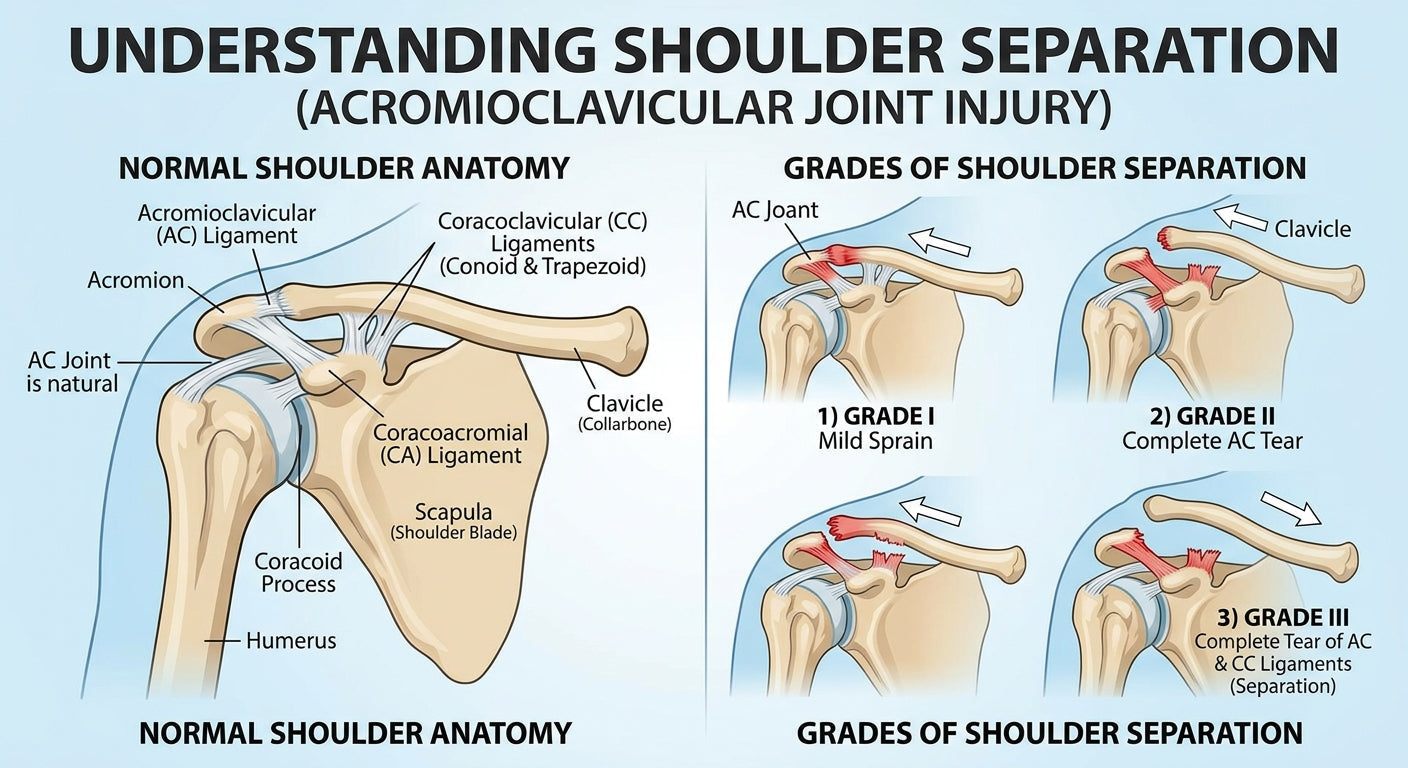
Shoulder separation, medically known as an Acromioclavicular (AC) joint injury, is a common ailment, particularly among athletes and individuals prone to falls. It occurs when the ligaments connecting the collarbone (clavicle) to the shoulder blade (scapula) are stretched or torn. Unlike a shoulder dislocation, which involves the ball-and-socket joint, a shoulder separation affects the joint at the top of the shoulder and often results in a noticeable bump.
What Causes a Shoulder Separation?
- Sports Injuries: Contact sports like football, rugby, and hockey, as well as sports that involve frequent falls, such as cycling, skiing, and wrestling, often lead to AC joint injuries.
- Falls: Direct impact to the shoulder, especially at the point of impact, is a primary cause.
- Accidents: Automobile accidents or other traumatic events can significantly affect the shoulder, leading to separation.
Recognizing the Symptoms
- Pain: Immediate and often severe pain at the top of the shoulder, particularly when moving the arm.
- Tenderness: The area around the AC joint will likely be very tender to the touch.
- Swelling and Bruising: Inflammation and discoloration around the joint are common.
- Deformity: In more severe cases, a visible bump may appear on top of the shoulder, indicating that the clavicle has been displaced upward.
- Limited Movement: Difficulty raising the arm above shoulder height or across the body due to pain and instability.
- Clicking or Popping Sensation: Some individuals may hear or feel a clicking or popping sensation during shoulder movement.
Understanding the Grades of Shoulder Separation
Shoulder separations are classified into different grades based on the extent of ligament damage and the displacement of the clavicle. This grading system helps healthcare professionals determine the appropriate course of treatment and predict recovery timelines.
Here's a breakdown of the typical injury grades:
 Compare injury grades side by side: clear guidance on when to choose conservative care vs. surgery, along with expected recovery timelines.
Compare injury grades side by side: clear guidance on when to choose conservative care vs. surgery, along with expected recovery timelines.
- Grade I: A mild sprain of the AC ligaments, with no significant tear or bone displacement. The joint remains stable.
- Grade II: A more significant sprain or partial tear of the AC ligaments, often with some stretching of the coracoclavicular (CC) ligaments. There may be a slight displacement of the clavicle, resulting in a small bump.
- Grade III: Complete tear of both the AC and CC ligaments. The clavicle is significantly displaced upwards, creating a noticeable bump on the shoulder.
- Grades IV, V, VI: These are rarer and more severe injuries involving complete ligamentous disruption and extreme displacement of the clavicle, often through muscle tissue.
Diagnosing a Shoulder Separation
A healthcare professional will typically diagnose a shoulder separation through a physical examination and imaging studies. They will assess tenderness, swelling, and range of motion. X-rays are commonly used to visualize the AC joint and determine the extent of clavicle displacement. Sometimes, special stress X-rays, in which a weight is applied, are taken to better demonstrate instability. MRI scans may be ordered to evaluate soft tissue damage, particularly to the ligaments.
Treatment Options: Conservative vs. Surgical
Conservative Treatment (Non-Surgical)
Most Grade I and II, and many Grade III, shoulder separations can be successfully managed conservatively. The primary goals are to reduce pain, minimize swelling, and restore normal shoulder function.
- Rest and Immobilization: Protecting the injured shoulder is paramount. This typically involves wearing an arm sling to support the arm and keep the shoulder still, particularly during the initial healing phase. If you're wondering how to heal a shoulder sprain, rest is often the first step.
- Ice and Pain Management: Applying ice packs to the injured area helps reduce swelling and pain. Over-the-counter pain relievers can also be used as directed by a healthcare provider.
- Physical Therapy: Once initial pain subsides, a rehabilitation program is crucial. This will involve gentle range-of-motion exercises, followed by strengthening exercises for the shoulder and surrounding muscles. Proper rehabilitation is key to regaining full strength and preventing stiffness.
- Supportive Devices: Various types of shoulder braces can provide additional support and compression, aiding in comfort and stability during recovery. An AC joint brace is specifically designed to help support the joint. For athletes, considering appropriate shoulder support for sports can be beneficial for returning to activity. You might find a suitable general option among various shoulder braces. For those concerned about re-injury, a shoulder brace for dislocation prevention can be considered.
Surgical Treatment
Surgery is typically reserved for severe Grade III injuries (especially in very active individuals or laborers), and all Grade IV, V, and VI separations where the clavicle displacement is significant, and stability cannot be achieved through conservative means. The goal of surgery is to reconstruct or repair the torn ligaments and stabilize the AC joint, returning the clavicle to its proper position.
- Common Surgical Techniques: These may involve using screws, plates, or strong sutures to hold bones in place while the ligaments heal, or reconstructing torn ligaments with grafts.
- Post-Surgery Care: After surgery, a period of immobilization, often with a specialized sling, is required. A comprehensive physical therapy program follows, similar to conservative treatment, but often with a longer and more gradual progression. If you have a rotator cuff injury, understanding when to use a sling for rotator cuff injury can also be relevant for general shoulder support during recovery. A shoulder brace for torn rotator cuff might also be used in some post-surgical rehabilitation plans.
Recovery and Rehabilitation
- Grade I & II: Typically, recovery involves a few weeks of rest and pain management, followed by several weeks of rehabilitation exercises. A return to light activities may occur within 2-6 weeks, with full return to strenuous activity potentially taking 6-12 weeks.
- Grade III (Conservative): Recovery can extend to 3-6 months for a full return to activity, with a longer period for regaining full strength and range of motion.
- Surgical Repair: While surgery aims to restore stability, the recovery period is generally longer and more intensive. Immobilization can last 4-8 weeks, followed by several months of physical therapy. Full return to demanding activities may take 6 months to a year.
Rehabilitation focuses on:
- Restoring the passive and active range of motion.
- Strengthening the rotator cuff muscles, deltoid, and scapular stabilizers.
- Improving proprioception (body awareness) and control.
- Gradual return to activity, often with sport-specific drills.
Preventing Shoulder Separation
- Proper Technique: In sports, learning and utilizing correct falling and tackling techniques can minimize impact on the shoulder.
- Strength and Conditioning: Maintaining strong shoulder and core muscles improves joint stability.
- Protective Equipment: Wearing appropriate padding in contact sports can offer some protection.
- Awareness: Being mindful of your surroundings to avoid falls, especially in high-risk environments.
-
Posted in
Shoulder pain








{kind=link}